The following manuscript is a shortened summary that accompanies the full OHBM ratified ‘best practices recommendations’ available online (https://doi.org/10.31219/osf.io/r7u8p). Amendments have been made to the present manuscript to incorporate additional reviewer feedback, leading to slight divergences when compared to the officially approved Best Practice Recommendations. A quick-reference summary is presented in Box 1; supporting evidence is detailed in the following document and the extended, uncut version. All appendices referenced in this manuscript can be found in the full document.
1. Introduction
The main clinical applications of functional MRI (fMRI) for individual patients include preoperative risk assessment and the mapping of “critical” cortex[1] for presurgical planning.1 Risk assessment refers to determining whether surgery will take place in the language dominant hemisphere, which entails greater risk for postoperative language impairments. Consequently, establishing how ‘strongly’ the targeted hemisphere is dominant for language informs patient consent, deciding whether to proceed with surgery, and the surgical plan itself. Presurgical planning also includes deciding on a strategy to reach a surgical target while minimizing damage to surrounding functionally important brain tissue. fMRI - if properly performed - allows the non-invasive visualization of gray matter functions at an individual patient level. But what constitutes ‘high-quality’ clinical fMRI?
The focus of most validation work on clinical fMRI has been mapping speech- and language-related functions, because their localization, with few exceptions (e.g., the ventral premotor cortex), cannot be accurately predicted from anatomy alone. However, despite ample reports highlighting fMRI’s value in guiding, selecting and tailoring neurosurgical interventions close to language regions, the application of fMRI for clinical language mapping remains controversial.2,3 While this controversy stems from several sources (including comparisons against other methods instead of patient outcome), one main challenge is the dramatic variation in approaches used in clinical language fMRI and, likely as a result, variability in outcomes.4
The biggest challenge for developing clinical guidelines to standardize practice is the large variety of tasks and methods4–7 used to conduct, analyze, and interpret clinical fMRI studies. Clinical language fMRI is more-or-less equal parts language neuroscience experiment, cognitive assessment, neuroradiological exam, image analysis application, statistical inference, and neurosurgical decision-making tool. The requirement for this range of complementary skills has meant that as fMRI has moved into the clinic, the discipline has fragmented among a range of professions seeking to characterize and standardize clinical fMRI from their unique perspectives,4,8 which may often mean a lack of interdisciplinary consensus.
In one early attempt at standardizing fMRI, neuropsychologists focused on the skills that valid clinical fMRI requires.9 A multidisciplinary approach was advocated, involving professionals with expertise in critical domains including (among others) cognitive and computer science, psychology, neuroradiology, neurology, and neurosurgery. In 2017, the American Society for Functional Neuroradiology (ASFNR) published recommendations for cognitive tasks used to map language functions in surgical patients. Perhaps in part due to the group’s neuroradiological focus, recommendations were based on a survey of tasks commonly in use at members’ institutions.7 In another report, the American Academy of Neurology summarized the quality of evidence supporting fMRI for lateralization[2] of language.5 When representative samples of individuals collecting and analyzing fMRI for epilepsy surgical programs were surveyed in the US4 and the EU,6 essentially all aspects of the procedure were found to vary.
The fMRI tasks and analysis approaches used are the most important aspects of clinical language fMRI to standardize to ensure best patient care. It may be of interest to know what tasks are in common use, but it is more critical to consider the validity of various practices. Several aspects of fMRI task design (e.g., sensory modality, control conditions) are important to explicitly consider due to their influence on the specificity of the activation patterns. In patients with existing language impairments, it may furthermore be necessary to alter task conditions, speed of presentation or difficulty levels, whereas ‘standard’ tasks have traditionally been ‘one-size-fits all’. From an analysis perspective, there is a lack of recommendations that address state-of-the-art data collection, preprocessing, analysis, and reporting. For example, in one clinical survey,4 the most used fMRI data smoothing kernel was 8mm, which happens to be the default setting in a prevalent data analysis package often used in neuroscience studies.10 Yet, default settings in research software are generally chosen with a different outcome objective in mind, namely to maximize group-level sensitivity by minimizing inter-individual variation in fMRI activation location and extent.11 In clinical settings, it is precisely the individual variability that we aim to capture because of its impact on surgical decision-making. Such technical and methodological considerations have profound implications for the interpretability of clinical fMRI2,3 and the spatial ‘localizability’ of findings.12
Through efforts by the Organization for Human Brain Mapping (OHBM) to improve best practices for neuroscientific imaging data analysis and reproducibility, Best Practices in Data Analysis and Sharing (COBIDAS) have been recommended.13,14 The OHBM Clinical fMRI Working Group was formed in 2017 in response to the specific challenges posed by clinical fMRI under the COBIDAS principles. This Working Group consists of a multidisciplinary committee spanning all domains of relevant expertise, including neurologists, neuroradiologists, neurosurgeons, imaging statisticians, neuroscientists, and neuropsychologists in both adult and pediatric populations. Bringing together practitioners from North America and Europe, the working group had two main goals:
-
To present the unique challenges of mapping language functions in clinical populations who frequently suffer from neurocognitive impairments; and
-
To put forward practical guidance for the acquisition, pre-processing, analysis, and reporting of individual patient data based on high quality research.
This document summarizes the main recommendations of the Clinical fMRI Working Group. Further in-depth considerations of the presented topics are provided in the full document (https://doi.org/10.31219/osf.io/r7u8p). In light of continued progress, especially with respect to technical aspects of fMRI data collection and analysis, it is hoped that these recommendations will improve minimum standards and facilitate meaningful use, enhance comparability between studies, and support large-scale evaluations of fMRI’s strengths and limitations in clinical practice.
2. Part 1. Clinical indications and approaches for fMRI language mapping
Due to the complexity of the language system, presurgical language fMRI starts by establishing the clinical question that fMRI is intended to answer. The following sections have been shortened; further nuances and supporting data are presented in the full document and its Appendices.
2.1. Inclusion / exclusion criteria and additional information required prior to fMRI
2.1.1. Patient selection
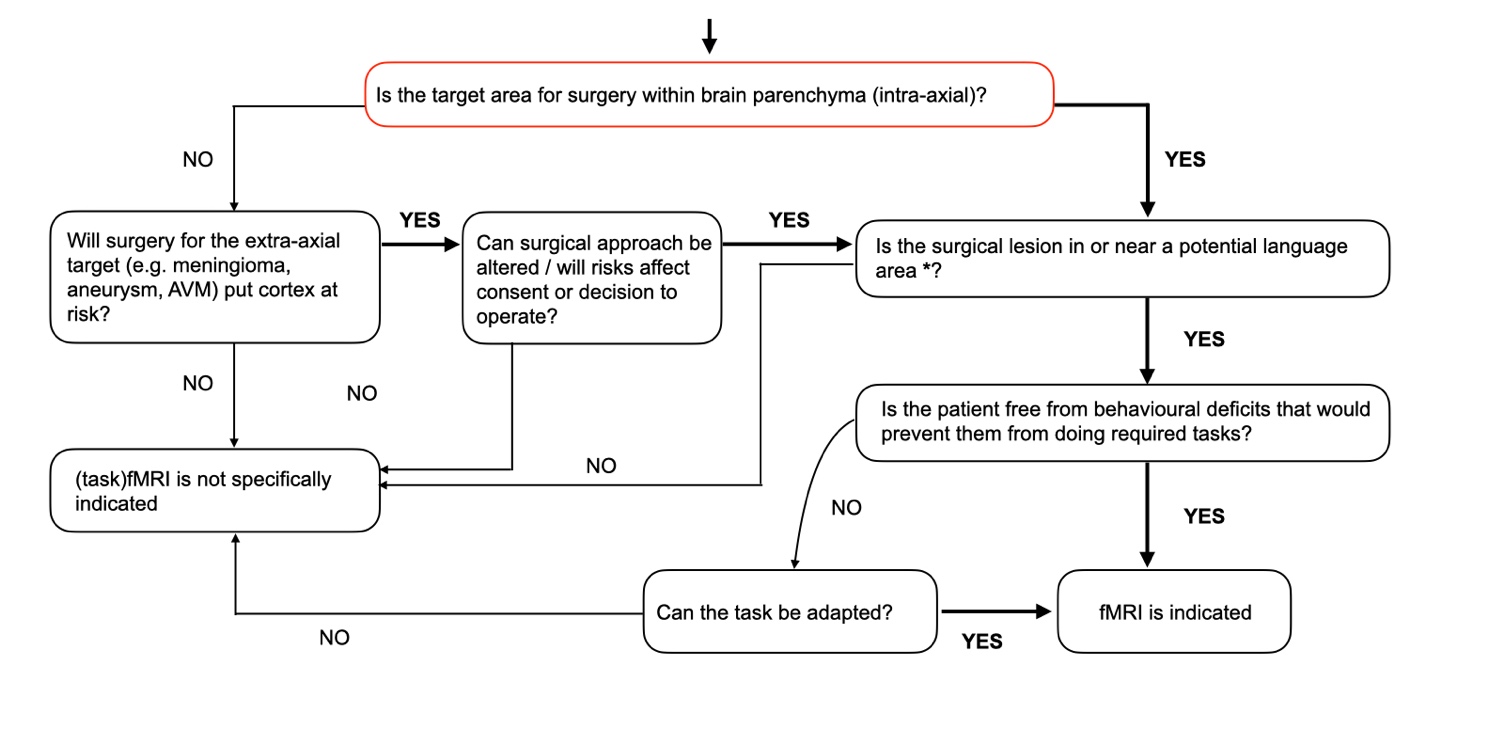
FMRI is primarily indicated for surgical targets within the brain parenchyma, i.e., intra-axially located, and where there is a risk of surgery causing language impairment. This risk may arise because the lesion is within or near functional cortex or associated white matter pathways. Alternatively, risks may exist when the surgical trajectory, e.g., a trans-opercular approach to the insula, could disrupt language networks. In selected extra-axial surgeries (e.g., resections of space occupying meningiomas, arteriovenous malformations (AVMs) with a nidus outside the brain parenchyma, or aneurysm clipping), language fMRI mapping can be helpful to inform surgical access and/or the temporal order of multi-stage embolization in relation to language territories at risk of hemorrhagic or ischemic damage15 (Fig 1).

2.1.2. Handedness & side of surgery
Numerous factors influence the risk that neurosurgery poses to language functions; one is handedness. The overall likelihood of atypical (i.e., ‘bilateral’ or right-hemisphere) language dominance is higher in left-handed or ambidextrous individuals (22-30%) than in right-handed people (4-12%) (e.g.,16–18). Still, the majority of non-right-handed individuals have typical left-hemisphere dominance for speech and language.19 Consequently, handedness alone is useful to inform, but not sufficient to rule out surgical risks. The incidence of atypical (bilateral or right-hemisphere) language dominance is higher in people with chronic epilepsy20,21 and some with a long-standing / slow-growing left hemisphere lesion (e.g.,22–24). Clearly, the consequences to the patient of removing potentially language-critical structures in the right hemisphere may be severe. A case can therefore be made for pre-surgical language fMRI if a surgical target, or intended access route, approaches possible language structures in either hemisphere.25
2.1.3. Cognitive status
Developments in resting state fMRI (rs-fMRI) offer promising opportunities for understanding the organization of functional networks without active patient participation, particularly in populations where task-based mapping is challenging26–31 (Appendix A of the full online report: https://doi.org/10.31219/osf.io/r7u8p). Rs-fMRI can provide valuable insights, particularly for assessing language lateralization or broad network organization. Indeed, it is widely acknowledged that functional networks extracted from rs-fMRI data typically correspond, at the group level, well with those from task-based fMRI. However, at the single-subject level, deducing the correspondence between a resting network and a specific cognitive function is less warranted, particularly in cases where – due to pathology – individual-specific organization can be expected to deviate significantly from a group-level organization of cognitive processing in the brain. For example, language laterality estimated from rs-fMRI has shown variable concordance (typically lower in patients than in controls32) and occasional misclassifications when compared to task-fMRI acquired in the same patients.33–35 Further validation of rs-fMRI is needed, as also highlighted in recent recommendations from the American Society for Neuroradiology,36 especially in relation to predicting individual patient language outcomes. Consequently, our consensus is that task-based mapping remains the most reliable method for identifying brain regions involved in specific aspects of language processing and that, currently, there is insufficient data to support the use of rs-fMRI alone for the purposes of mapping language processes whenever a task can be acquired.
However, task-based fMRI is often not feasible in patients who are unable to cooperate or tolerate MRI, including very young children (typically < 6 years, depending on the child) who may require sedation to undergo MRI. In select adult cases and very young children, rs-fMRI or passive tasks (e.g., sentence or story listening) may serve as useful adjuncts, particularly when adapted to the developmental and clinical context. However, there is a paucity of studies in infants assessing – with any technique – the lateralization or localization of language functions.37 There is similarly insufficient data reported in wider populations unable to tolerate task-based fMRI to guide specific recommendations. A small number of studies have attempted to determine language lateralization from fMRI acquired in children under deep sedation. The largest study to date concluded from the much higher rate of ‘atypical’ (bilateral) patterns that “language patterns observed in a sedated fMRI with passive task may not truly represent the language networks of wakefulness”.38 In children under <5 years, language networks may not be fully established and activation patterns may be particularly modulated by language abilities,37 adding interpretational confounds to maps without active participations and performance read-outs.
Since our recommendations were created in the context of mapping speech and language-related functions with task-based fMRI for specifically indicated purposes and populations (Fig 1), we are not able to put forward consensus recommendations outside of those applications and populations, i.e., for use in individuals (child or adult) unable to actively participate in task-based fMRI. In such cases, alternative methodologies for functional localization and/ or lateralization with e.g., ESM, electrocorticography, transcranial magnetic stimulation, functional near-infrared spectroscopy and functional transcranial doppler ultrasonography may have complementary roles. Yet, as with fMRI, further data are needed around the contribution of each of these methods to predict language outcomes in these populations.39
For all these reasons, appreciating the detailed neurological and cognitive performance status of each patient is essential when planning language fMRI. In some patient groups, such as those with temporal lobe epilepsy, use of pre- and post-operative cognitive assessment batteries is well established and predicts whether dominant left temporal patients are at low, medium, or high risk of post-surgical naming decline.40 In other populations, such as high-grade gliomas, pre-operative performance is not routinely captured. However, impairments may prevent patients from completing meaningful fMRI. There is little benefit to be gained, for example, by attempting fMRI language mapping when the patient is too aphasic to comprehend instructions, or tasks are too difficult for them (see 2.3.6). As a minimum, potential patients should (a) be co-operative and able to tolerate being in a noisy, confined space while performing fMRI tasks and (b) have minimum abilities to both perform required tasks and simultaneously avoid certain behaviors (e.g., moving or talking out loud during the task, if silent responses are required). Neuropsychological assessment can (1) detect subtle deficits not apparent conversationally but predictive for surgical risks; (2) identify the need for modifications to fMRI tasks; (3) identify wider attention/memory difficulties that may affect fMRI performance. It is also important to consider deviations from age-typical milestones (whether precocious or delayed) for appropriate task selection in pediatric patients (see full document). Consequently, best practice is to establish neuropsychological performance before fMRI and surgery, and again post-operatively to evaluate outcomes. Short (e.g., bedside) testing of primary cognitive and language domains, along with some more targeted in-depth assessment of deficits, is generally feasible in virtually every case.
2.1.4. Contraindications
Absolute and relative MRI contraindications apply, while important confounds limit fMRI interpretability, considered in the full document and accompanying Appendix B.
2.2. Clinical objectives of presurgical fMRI language mapping
Objectives of speech and language fMRI mapping generally separate into inter-hemispheric lateralization versus localization of functional tissue. Tasks optimized to lateralize language can be less suited to localize functions, and vice versa. Consequently, precision in formulating the clinical request and surgical goals helps with tailoring tasks to maximize fMRI’s utility.
2.2.1. Lateralizing language functions
Risks of developing postoperative language and verbal memory deficits is partly dependent on language lateralization .5,40 Language lateralization using fMRI has been most extensively assessed prior to temporal lobe surgery to treat drug-resistant epilepsy.21,41 The clinical purpose is usually to establish graded language lateralization as an alternative to invasive Wada testing.42 Laterality results are often used to inform consent and/or tailor the surgical approach / extent. Laterality can also be useful to (re-)establish in patients who have undergone previous surgery, in whom inter-hemispheric language dominance may change through functional reorganization.22
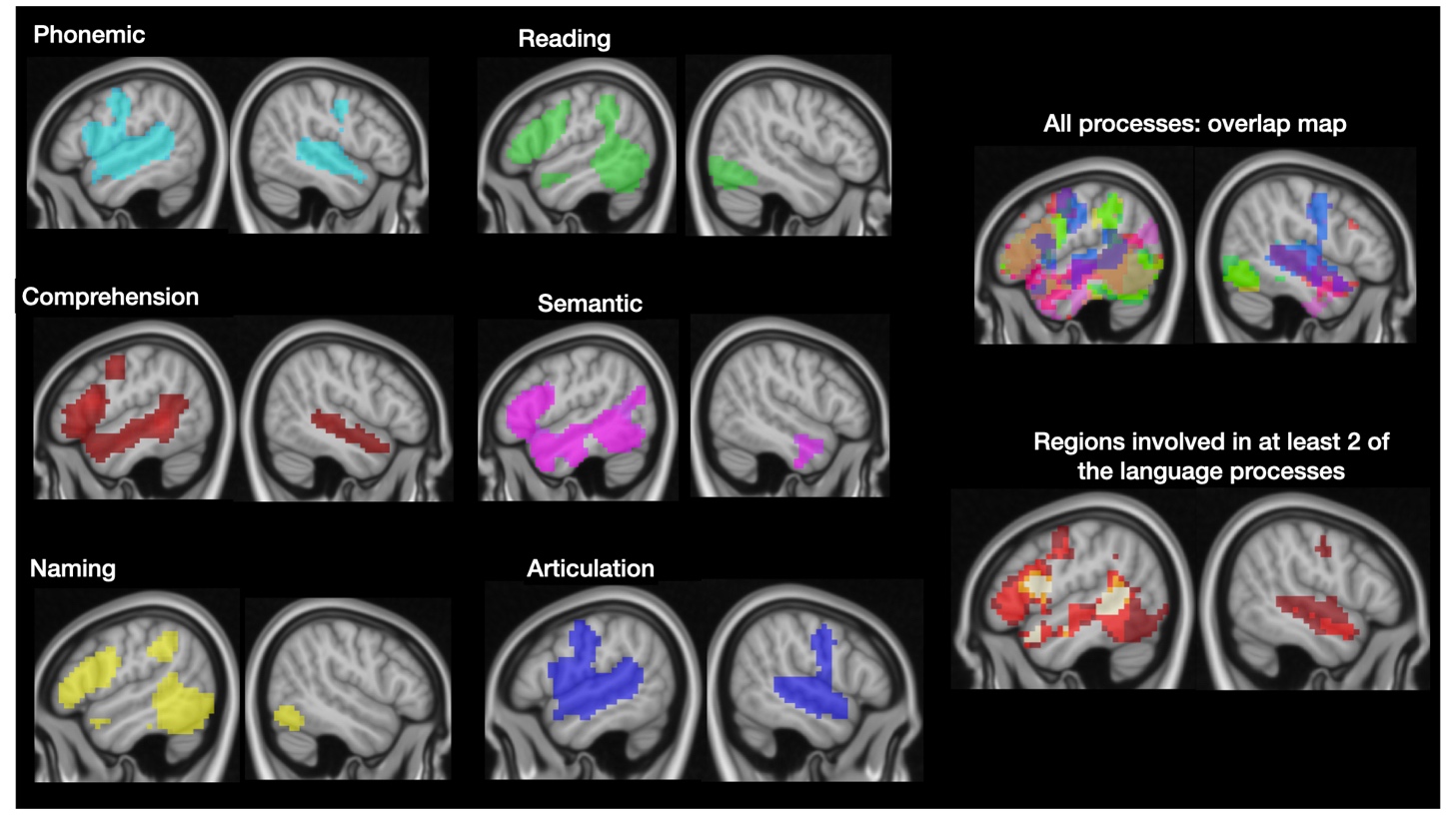
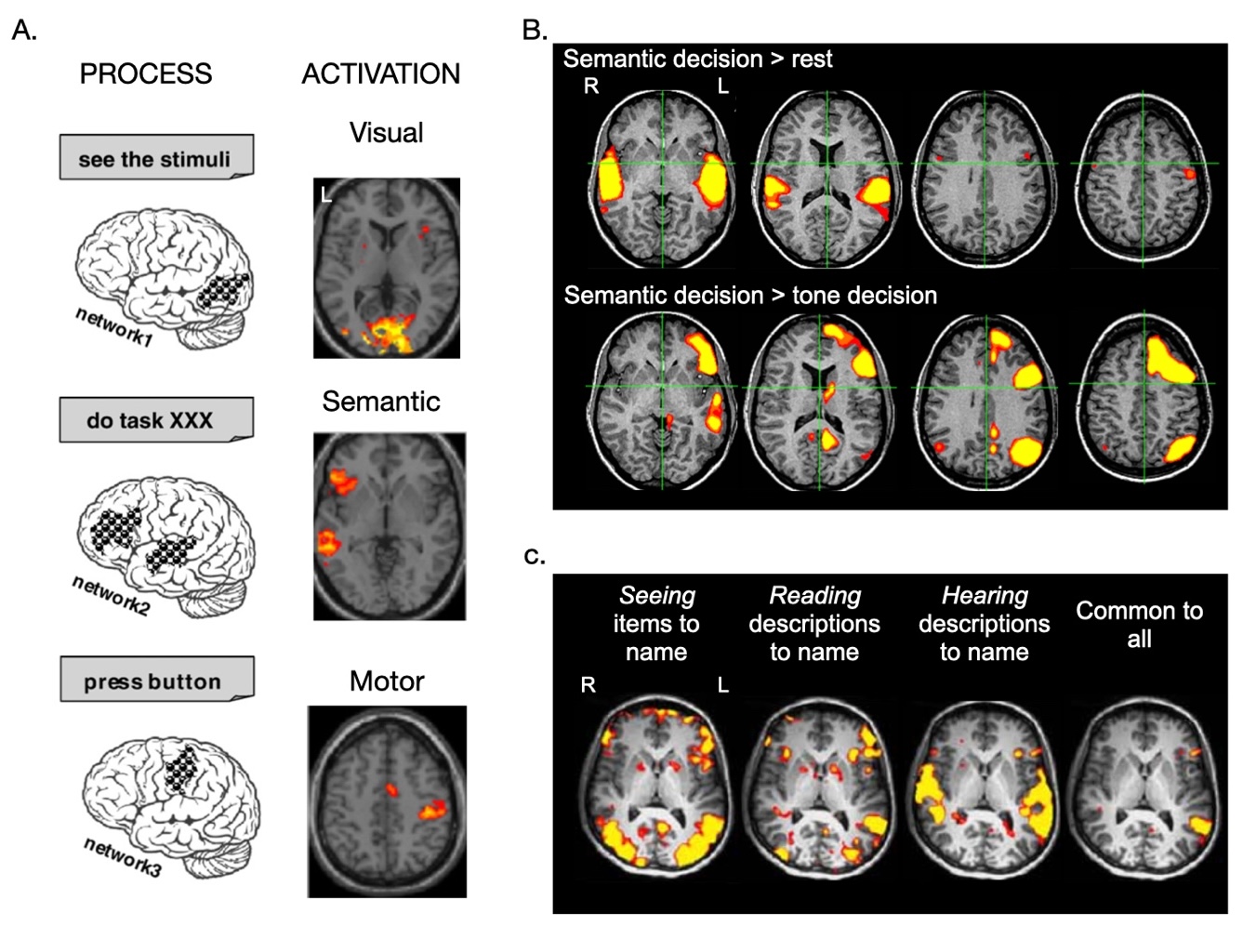
In terms of the task approach, different tasks engage different parts of the language system to variable extents (Fig 2). Within the same patient, the left and the right hemispheres can both participate in - and rarely even be “dominant” for - different aspects of language (so-called “crossed dominance”).43 Consequently, a combination of task contrasts assessing an array of language functions are generally advocated to establish laterality at the lobe-level.43–47 Surveys4,6,48,49 indicate that epilepsy surgery and glioma-specialized centers typically assess language lateralization using at least two, and routinely 3 or more fMRI tasks.

In addition to the type of language task, laterality results are strongly influenced by specific paradigm choices regarding control conditions, i.e., what the language task is compared against.42,50,51 For example, comprehension tasks presented in the auditory modality offer poor lateralization if (the strongly bilateral52) acoustic processing is not accounted for. Similarly, multiple studies emphasize the importance of controlling for nonlinguistic aspects of language processing (e.g., using non-language visual or auditory decision tasks) to lateralize semantic processing in the temporal lobe.50,53 Establishing regional laterality therefore requires careful consideration of both the task’s active and control conditions.
General approaches to establish language laterality are presented in Box 2. Of note, establishing lateralized representations of language functions does not exclude the possibility that an area of detected activation in the “non-dominant” hemisphere may be indispensable to language.54 The “size” of an area of activation as detected by fMRI strongly depends on statistical analysis and thresholding of the data (section 3.3) and does not, per se, reflect its functional importance. Consequently, surgically-oriented applications of fMRI are more often concerned not only with establishing which hemisphere harbors language functions, but also with identifying where they are located and what language functions are most at risk.
2.2.2. Localizing language: functions of concern in specific brain areas
Functional MRI efforts to localize language centers in relation to a focal lesion are intended to:
- predict the specific risks associated with the surgery,
- facilitate informed consent,
- provide an estimate of likely resectability / achievable resection extents,
- plan the surgical approach and / or
- guide the need for / use of Wada or intraoperative electrocortical stimulation mapping (ESM).
Among surveyed centers, almost 80% of neuro-oncology respondents use fMRI to localize language functions,49 with 88% requesting fMRI to help inform extents of resection.68 Some 44% of epilepsy centers already cautiously use fMRI to guide surgical margins.69 Suitability and limits of fMRI used for these purposes are difficult to evaluate. There is limited data systematically evaluating language outcomes, and high variability in how language is assessed both with fMRI and intra/peri-operatively. What is clear, however, is that clinical applications of fMRI to help decide ‘is this area safe to ‘cut’?’ generally require several carefully controlled tasks to isolate different aspects of language processing according to the structures most at risk in a given surgery.
Optimal fMRI tasks and task designs for language ‘localization’ remain an open question. In selecting an approach, recent reviews of widely used tasks can be found in references 4,51,70–72. Users could also consult large-scale neuroimaging database resources to observe the typical activation patterns of specific language tasks / processes (e.g., Figs 2, 3). Ultimately, however, fMRI task selection should draw on knowledge of the role of specific brain regions in essential aspects of language processing.45,73–75

Data supporting a role for certain brain structures in aspects of language have been widely replicated over the past 30 years.73 Questions surrounding language localization predominantly arise in the context of surgery involving:
- the inferior frontal gyrus (IFG),
- parts of the (especially posterior) middle frontal gyrus (MFG),
- posterior middle and superior temporal gyrus (MTG/pSTG) and sulcus (pSTS),
- inferior parietal lobule (IPL) and
- the mid-fusiform gyrus / basal occipitotemporal cortex.
Language-related deficits are also associated with surgery involving the supplementary motor area (SMA) and pre-SMA, but are mostly transient if the contralateral homologue can support this function76 and if the corpus callosum remains intact. Additional brain regions, including the temporal pole, the graphemic motor area (aka Exner’s) and Hopf’s area 55, contribute to language in ways that remain incompletely understood and are therefore challenging to ‘map’ (see full document).
In order to help preserve function after surgery, the aim of clinical fMRI is not to just activate a specific brain region, but to identify the network or assembly of brain regions engaged during specific language processes. This distinction is important for two reasons, which boil down to:
-
Several neuronal populations contribute to more than one function, and
-
'Language’ is not a single unified behavior. Brain regions that each perform more or less specialized computations likely combine in specific ways to support particular ‘language’ requirements.77,78
The 'core’ set of processes required for different aspects of language79 includes a) semantic access (knowledge of concepts and meaning), b) phonological representations (the sound of words), c) lexical access (our store of learned vocabulary), d) orthographic and graphemic knowledge (visual word recognition and spelling), and e) syntax (knowledge of the rules governing word order and the functional roles of words in language). Speech generally requires articulation (planning, coordination and programming of speech), which is necessary but not specific to spoken language.80,81 At present, there remains uncertainty as to the level at which syntactic processing is supported by a neurally-distinct network in the brain,82 and about the neural substrates for temporal /syntactic order predictions (e.g.,83–85). Other cognitive processes also directly influence language performance.86
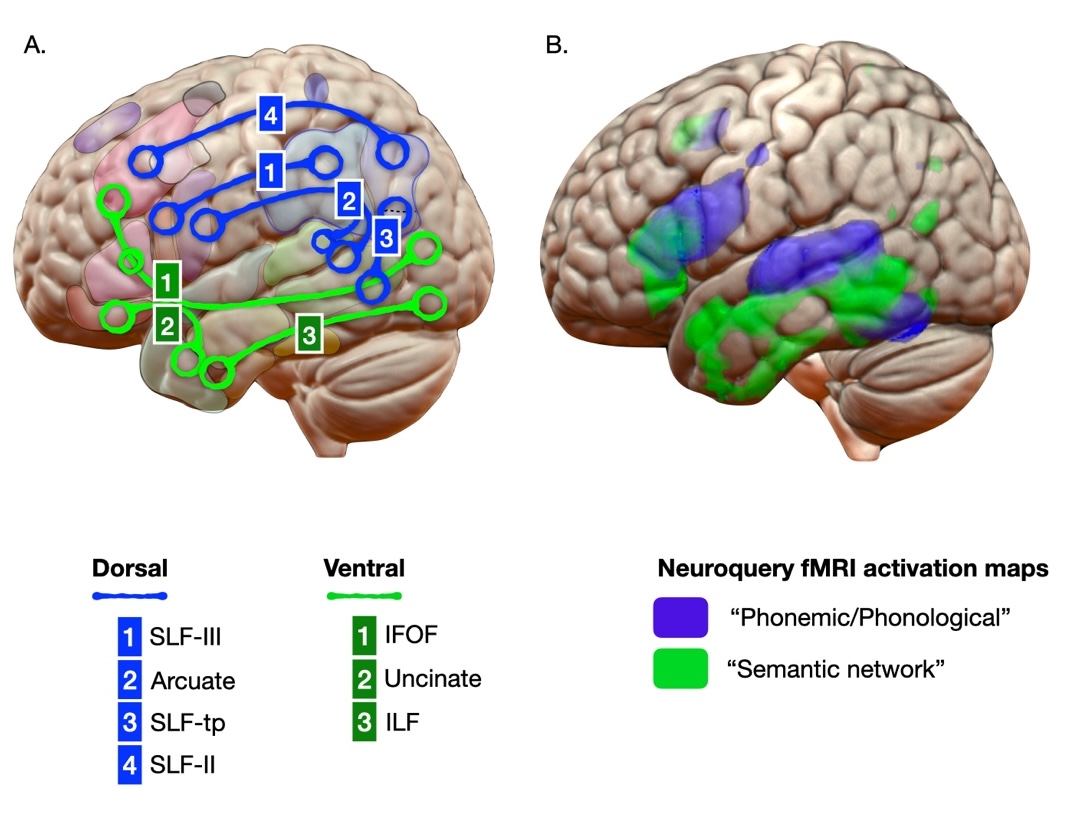
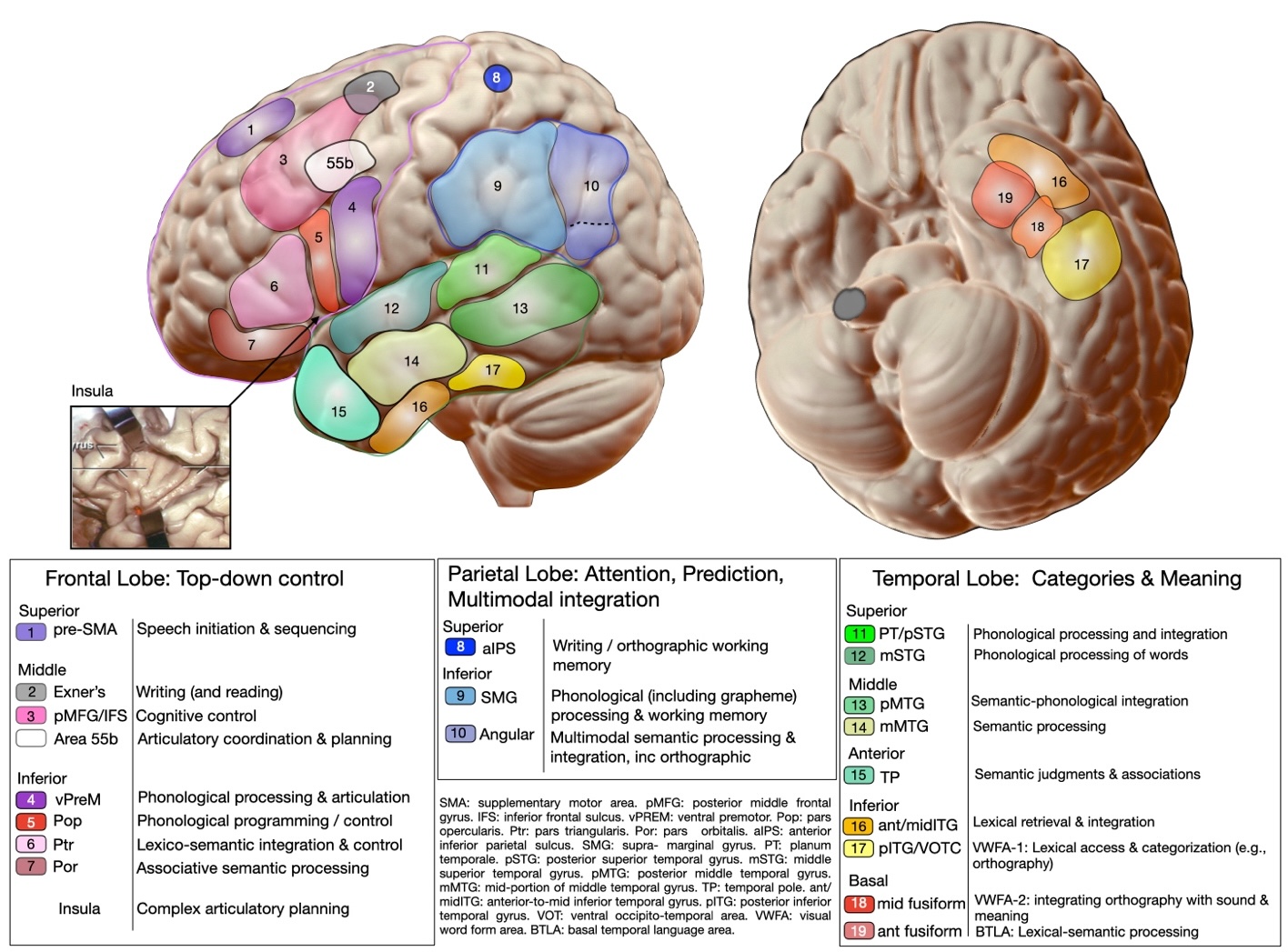
These ‘core’ language processes are often described in terms of (at least partially) discrete networks consisting of (at least partially) separate brain regions. The current dominant theory suggests two large-scale interacting systems87,88; one supporting conceptual (lexico-semantic) aspects of language and the other supporting phonological processing and speech.89,90 Fig 3 illustrates this dual stream model, presented alongside statistical maps of cortical brain regions activated during ‘semantic’ and ‘phonemic’ language processing according to predictive modeling of results from 13,450 neuroimaging studies in Neuroquery.91 Mapping specific language processes onto the dual-stream model is complicated by the fact that most language tasks evoke the functions supported by both streams to varying degrees. Additionally, many of the pioneers of language localization theories observed that focal ‘deficits’ (or stimulation-induced disruptions in the case of Penfield) likely reflect disruption to a wider language network.92 Anomia, for example, is among the most frequently observed language deficits, but can result from disruption of several non-overlapping regions in the language-dominant hemisphere.78,79 That is, the task of naming is not ‘localizable’ per se.93,94 Nevertheless, converging data from stroke93,95 and resection outcome studies96,97 indicate that some brain regions appear to contribute more critically to language than others78,79,93 (Table 1). Allowing for our still-evolving understanding, Fig 4 summarizes the general approximations of core function-to-anatomy language mappings that are considered ‘reliable’ based on converging lesion, brain stimulation and imaging data (noting this is just one of different possible conceptualizations). Accordingly, the language processes most relevant to consider, and tasks commonly used to delineate them, are outlined in Table 2. When considering the tasks in Table 2, it’s essential to recognize variability in the effectiveness of theoretically appropriate language tasks. Some tasks demonstrate greater validity and reliability than others.98,99 Optimal tasks (i) reveal lateralization effectively, (ii) activate relevant language regions (validity) in a higher percentage of patients (reliability), and (iii) produce consistent maps across sessions (test-retest reliability). For example, semantic decision tasks generally yield stronger lateralization and more reliably activate frontal and temporal language regions than picture naming.98

2.3. Design and Paradigm considerations
2.3.1. Maximizing sensitivity
Once the precise clinical question and target language processes have been identified, the sensitivity of fMRI will be influenced by how easily the language-related signal of interest can be distinguished from a comparison baseline signal (e.g., ‘rest’ or active ‘control’ conditions). When the aim is to capture the neural activity associated with a general task (naming, for example) but the specific responses (e.g., individual objects named) are not crucial, a simple ‘block design’ is favored because it maximizes sensitivity to detect average BOLD responses.101 Using block designs, one or more language functions can be mapped in a relatively short experiment, making this the most prevalent design in clinical use,4 despite limitations, such as assuming a sustained BOLD response throughout each task block.
For some tasks, the objective is to isolate correct responses (e.g., only items named accurately). In these cases, capturing the neural response at precise timings is important, which requires ‘event-related’ analyses. The increased precision of event related designs, however, comes at the cost of reduced statistical power101 and requires longer acquisition times to reliably estimate overall neural responses, especially if there is a low(er) number of successful trials. Event-related designs are therefore not typically employed for clinical language mapping. However, further research into the potential benefits of ‘mixed’ block and event related designs is warranted.102
2.3.2. Advantages of a task panel approach
Variations in task demands affect both within-hemisphere localization and lateralization. When the clinical objective is to establish language laterality, as mentioned, a standard panel of tasks can generate language maps in the language-dominant hemisphere that are superior (i.e., more ‘complete’) to those generated with a single task45,103–105. Because location and extent of activation for any language task depends as much on the chosen control condition as on the language task itself, it is highly recommended to conceptualize task protocols in terms of task contrasts rather than isolated tasks. When the clinical objective is to localize specific language-related processes around a surgical lesion, therefore, a tailored task panel approach, contrasting different conditions, is typically needed to adequately probe all language functions at surgical risk. Mapping distinct language processes could theoretically be achieved using a single paradigm containing multiple active conditions / task contrasts. However, there are advantages (e.g., minimizing movement) to employing short, targeted task contrasts, each separately assessing a given language process at risk. Further empirical data are needed to support the use of specific tasks over others for a given language process/region, but various options are listed in Table 2.
2.3.3. Optimizing specificity
2.3.3.1. Many-to-one processing
Neuroscientific and lesion-based evidence indicates that multiple cognitive processes can engage a single brain region; so-called ‘many-to-one mapping’.106 Choosing appropriate tasks – and task contrasts – that selectively engage individual brain regions is therefore a challenge. Within this constraint, general approaches are considered next.
2.3.3.2. Selecting task ‘control’ conditions
‘Resting’ remains a common baseline condition in clinical fMRI designs4 and is implemented in many commercial task-fMRI protocols that compare blocks when the task is ‘on’ versus ‘off’ (i.e., during rest). Pitfalls of using ‘rest’ as a comparison baseline have been highlighted previously.107 ‘Rest’ is an uncontrolled state108; important functions take place during ‘rest’, including memory consolidation108 and internal cognitive and linguistic processes,109 even when the ‘rest’ periods are very short (e.g., 3 seconds).108 Consequently, using ‘rest’ as the comparison in a language task limits sensitivity for detecting activation in language-related networks. Fig 5b shows the effect on a semantic decision language activation map just by varying the control condition from ‘rest’ to auditory tone decision. To increase sensitivity and specificity, carefully designed comparison conditions should aim to ‘control’ for aspects of task performance that co-occur with the language process of interest.110

The choice of which control conditions to use is often a balance of specificity against sensitivity and clinical feasibility. Most commonly, the aim is to map complementary language processes using individual language tasks that will be analyzed separately. In this case, the choice of control condition in each task should reflect the desired level of precision in mapping each function (Table 2). Considerations are listed in Box 3.
2.3.4. Pre-fMRI practice session:
A recent survey indicated the most frequent reason for inconclusive language fMRI results was inadequate patient performance (47.3%),6 yet most participating centers spent <15 minutes on patient practice (55%) or gave no pre-scan instruction at all (14%). The Working Group strongly recommends a practice session with the patient prior to fMRI, to ensure they understand and are able (with appropriate modifications where possible) to perform the task as required, know when and how to make any required responses, and understand the problematic nature of head movements (further details: https://doi.org/10.31219/osf.io/r7u8p). For adults, preparation could consist of online training materials (e.g., stanfordhealthcare.org/fmri),116 supplemented with essential in-person practice. For pediatric patients, virtual and in-person MRI simulator sessions (e.g., https://www.bcchr.ca/3tmri/facilities/about-simulator) are recommended where possible to maximize success.
2.3.5. Modifications for patients with specific impairments
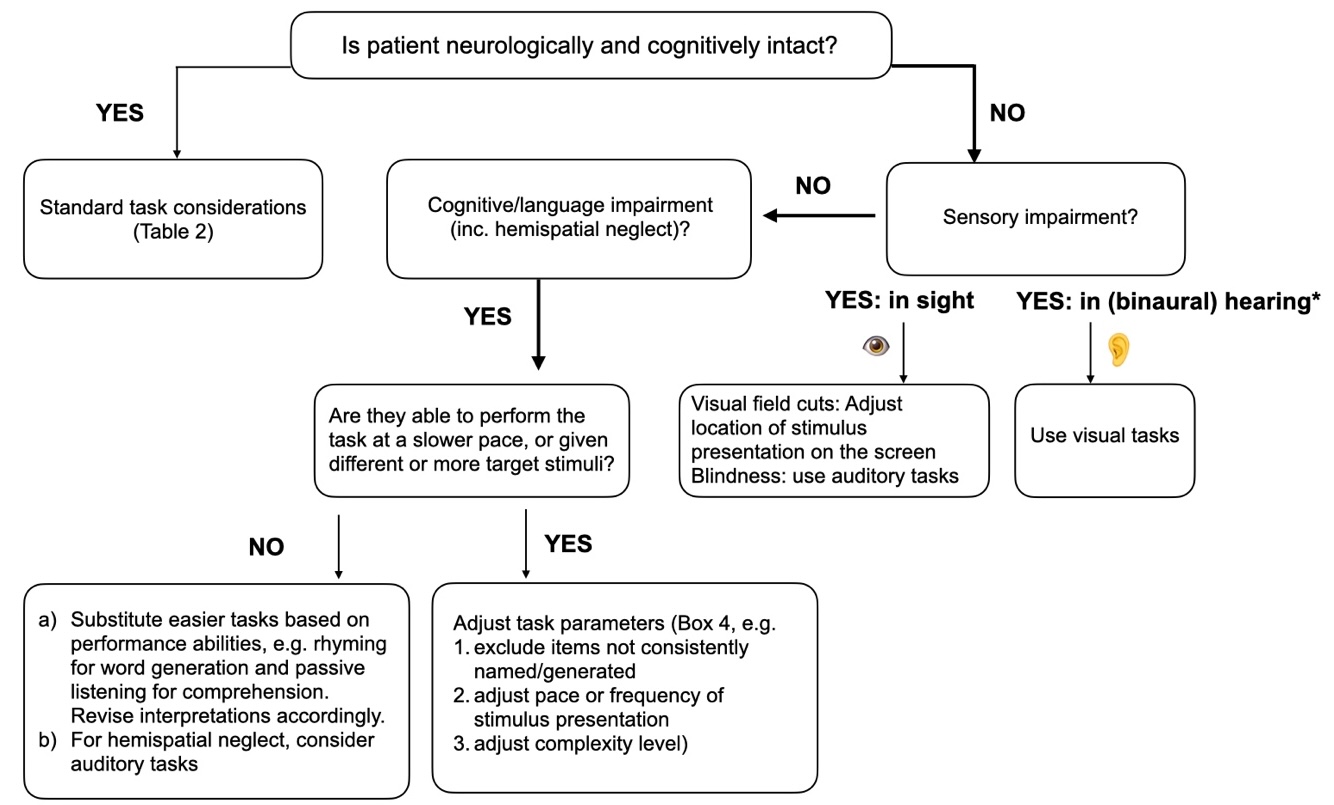
Specific considerations arise in populations presenting with various degrees of language deficit (Fig 6 and Box 4 of the full document).

2.3.5.1. Task modality
Language task stimuli are most frequently presented visually.4,7 For patients with difficulties processing certain types of stimuli (e.g., written words in dyslexic or alexic individuals), or uncorrectable vision impairment, it may be necessary to change the modality of stimulus delivery (e.g., to auditory cues or picture cues) for language mapping to succeed (Appendix C).
2.3.5.2. Task speed & difficulty
Task difficulty influences fMRI activations in numerous language tasks.114,117–121 It is important to ensure a patient can perform the task over the entire session while keeping the task challenging enough to maintain continuous engagement (and minimize mind-wandering). However, when task performance becomes too difficult, the same regions can show less activity, indicating a relationship (often shaped like an inverted ‘U’) between task difficulty, cognitive effort, and BOLD response.122,123 Together, the data suggest that tasks should be optimized for patient performance - hard enough to require cognitive effort, not so difficult that the patient disengages altogether. A recommendation in patients with existing language impairments is to maintain a balance between accuracy and motivation by targeting ~70-80% performance accuracy.
Among our Working Group, some employ pediatric versions of a task in adult patients with aphasia or impaired speed of performance. Others have had good results with protocols developed for aphasic patients, such as Adaptive Language Mapping (ALM).98,124 ALM adjusts task difficulty on-line – based on performance – (https://aphasialab.org/alm/), using psychometric properties that have been quantified. ALM therefore offers an evidence-based approach, which, in one study, provided more robust laterality indices and stronger extents of activation than widely used clinical paradigms.125 When task modifications are not feasible on a per-patient basis (e.g., because of lack of options in certain commercial software packages), it becomes even more important to establish, through cognitive evaluations and pre-scan practice, that patients can perform adequately.
2.3.6. Considerations for pediatric patients
A study of over 400 language fMRI scans in clinical child populations indicated an overall promising success rate of fMRI, but a higher rate (~15.8%) of ‘failed’ scans when compared to typically developing children.126 Predictably, ‘failed’ scans increase with lower age127 and is driven primarily by head motion, which can be mitigated. 128,129. Scan failures are also attributed to some children falling asleep.126 These findings emphasize that children may benefit particularly from task modifications that a) sustain attention and effort using several (short) tasks, and b) ensure a minimum number of successful responses.130 Clinical fMRI is generally more successful in children > 7 years old .126 It is recommended to use at least 3-4 short tasks,44,131 partly because head motion increases with every additional minute of acquisition.132 Activation procedures should be individually tailored according to performance level (as for adults), but also according to developmental stage.44,133 This is because non-linguistic ‘difficulty’-related contralateral activations likely drive an increase in apparent ‘bilaterality’ in some fMRI tasks relative to language lateralization results from Wada testing.131 Selecting an active comparison condition is especially beneficial to maintain attention and engagement in younger children who are less able to comply with the requirements of ‘resting fixation’134 and/or children with neurodevelopmental and behavioral disorders (considered in135). Making the scanning environment easier for children, through mock sessions or training, can be beneficial for increasing compliance with task-based fMRI. Strategies such as using favorite toys or playful scenarios (e.g., imaging the MRI as a spacecraft) may also help engage the child and reduce anxiety. These considerations highlight the need for flexibility and case-specific strategies in surgical planning.
A very wide range of tasks and task contrasts has been described for pediatric language fMRI. Data showing probabilistic activation maps or comparisons between these tasks in terms of lateralization or activation pattern in children remain lacking. When considering an optimal battery of pediatric language fMRI tasks, one solution is to employ a different panel of tasks best suited to specific age ranges. The main drawback of such an approach is that the interpretation of results between different age groups, and, importantly, in the same child over time, becomes challenging.136 An alternative solution is to adopt a single battery of tasks, in which each task aims to engage a specific language process (e.g., phonology, semantic retrieval, …), using parallel versions that vary in difficulty level. Specific task considerations are discussed in the full document: https://doi.org/10.31219/osf.io/r7u8p. Further development is advocated to establish age-appropriate naming stimuli and norms in pediatric populations.137 An additional consideration is that pediatric language mapping may be influenced by higher brain metabolism affecting the measured BOLD signal.
2.3.7. Bi- and multilingual patients
In bilingual neurosurgical patients, in addition to brain regions that are shared, separate areas of cortex uniquely subserve the primary versus additional languages138 (see full document). Language fMRI mapping should prioritize the primary language, but should ideally include all languages used by a patient in their everyday life.
Certain tasks, such as silent object naming, can be administered in multiple languages without the need to modify stimuli. However, cultural differences in familiarity with certain stimuli may affect performance. The difficulty of other tasks, such as phonemic fluency, depends on the frequency of individual letters in different languages, which should be chosen according to available normative data (i.e., appropriate ‘difficulty’ level) in each language. Several common paradigms are available in multiple languages as part of some commercial packages, or freely from research groups (www.cogneuro.net/hbm201775). Several participants of the Working Group employ parallel language versions of tasks, especially for reading and comprehension tasks.
Over and above possible differences in the brain regions supporting language production, speakers of multiple languages make use of a distributed ‘control’ network.139–141 Damage to this network can result in uncontrolled fixation to a single language142,143 or mixing/switching of languages without aphasic symptoms.144,145 Therefore, a language switching task is useful to consider when undertaking language fMRI mapping in bilingual patients .139 Perhaps the simplest would be word translation (present word in one language and request a response in another language), or alternating language blocks (e.g., using a country flag to indicate the target language146).
3. Part 2. Acquisition and analysis of clinical fMRI data
3.1. Skills & training
While fMRI is sometimes considered a standard neuroradiological exam, it is not. Clinical language fMRI is a form of cognitive assessment and requires case-by-case input from experts in multiple domains.9 Professionals with extensive multidisciplinary training in clinical fMRI, or pairs with complementary training are needed for optimal patient care (see https://doi.org/10.31219/osf.io/r7u8p). It is beneficial if the same specialist practitioner can accompany the patient through the multiple stages of the process (i.e., pre-op and follow-up evaluations, fMRI, and intra-operative assessment if performed).
3.2. Data acquisition
Technical aspects of MRI data acquisition and processing impact on the success and utility of clinical fMRI (summarized in Box 5 of the full document, here: https://doi.org/10.31219/osf.io/ r7u8p). Among the most critical recommendations is to monitor the success and quality of fMRI exams in real time and seek feedback from patients after every fMRI run, so that any apparent problems (e.g., motion or inadequate task compliance) can be addressed.
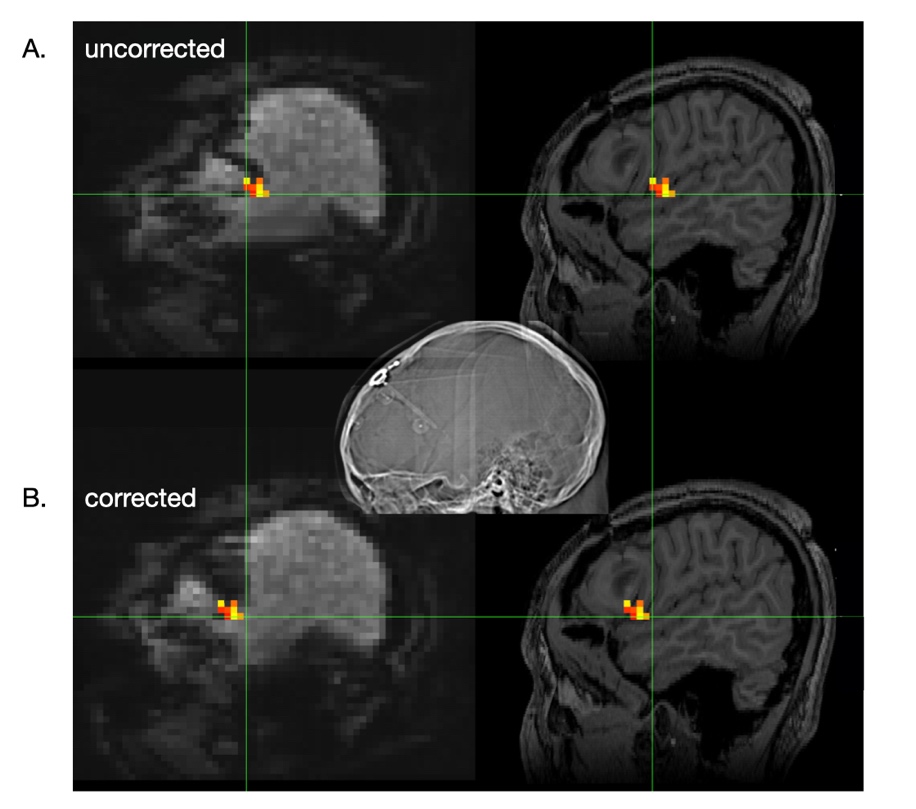
Performing task fMRI requires dedicated hardware. A combination of visual and auditory tasks allows for more comprehensive mapping of language networks than tasks delivered in only one modality (e.g.,52,53,62,147), as also reported for intraoperative stimulation mapping.148 Dedicated equipment and sequence properties are considered in the full document. It is recommended that additional field mapping sequences are acquired for subsequent correction of EPI distortions and accurate alignment to non-EPI (e.g., T1) data (Fig 7).
As part of fMRI scans, complementary acquisition of diffusion (tensor, or ideally more advanced) imaging to reconstruct fiber tracts involved in speech and language processing is recommended (Appendix D). Cerebrovascular reactivity mapping can additionally be considered (Appendix F).

3.3. Analysis
Unlike structural MRI, it is not the acquired fMRI-BOLD images themselves, but the statistical results generated from them upon which clinical interpretations are based. Choices in processing and statistical analysis can fundamentally impact results, revealing or obscuring task-related signal. Comprehensive reviews have detailed imaging analysis ‘best practices’ for the general neuroimaging community.13,149,150 However, decisions relevant to analyzing individual patient data differ in important ways from guidelines that apply to group analyses. A few select processing choices that particularly impact on the interpretability of single-subject clinical fMRI results are considered below (summary in Table 3 of the full document). The single most important recommendation is to undertake quality control at every step.
3.3.1. Head motion and motion correction
Language tasks, especially those involving overt speech, are particularly prone to stimulus- or task-correlated motion. Objective criteria for how much head motion is “too much” cannot be easily established, but in the worst case, head motion can make brain activation uninterpretable. The best and most effective approach for dealing with head motion is prevention, often readily achievable through careful patient preparation and real-time inspection of the images so that scans can be repeated, if required, before the patient leaves the scanner. Various strategies to ‘correct’ head motion exist151 (Appendix E) and practices vary widely. This group’s consensus is that neither prospective nor retrospective motion correction should be assumed to fix all issues arising from head motion. Subject head motion should be assessed in each fMRI scan through a variety of means. This includes inspection of the raw images and retrospective motion correction / realignment plots, as well as performing multiple analyses to compare the effects of different motion correction choices on the resulting activation maps.
3.3.2. Brain extraction and statistical mask generation
Some data pre-processing pipelines remove non-brain tissue (eyes, orbits, skull and dura) from the images. This step can have the unintended effect of also removing low-signal lesions and their perilesional areas.152 If brain extraction/mask generation is part of the initial processing pathway, it is crucial to verify that brain extraction has not also excluded the pathological lesion and the area around it from statistical analysis and, if necessary, edit or replace the brain mask.
3.3.3. Spatial Smoothing
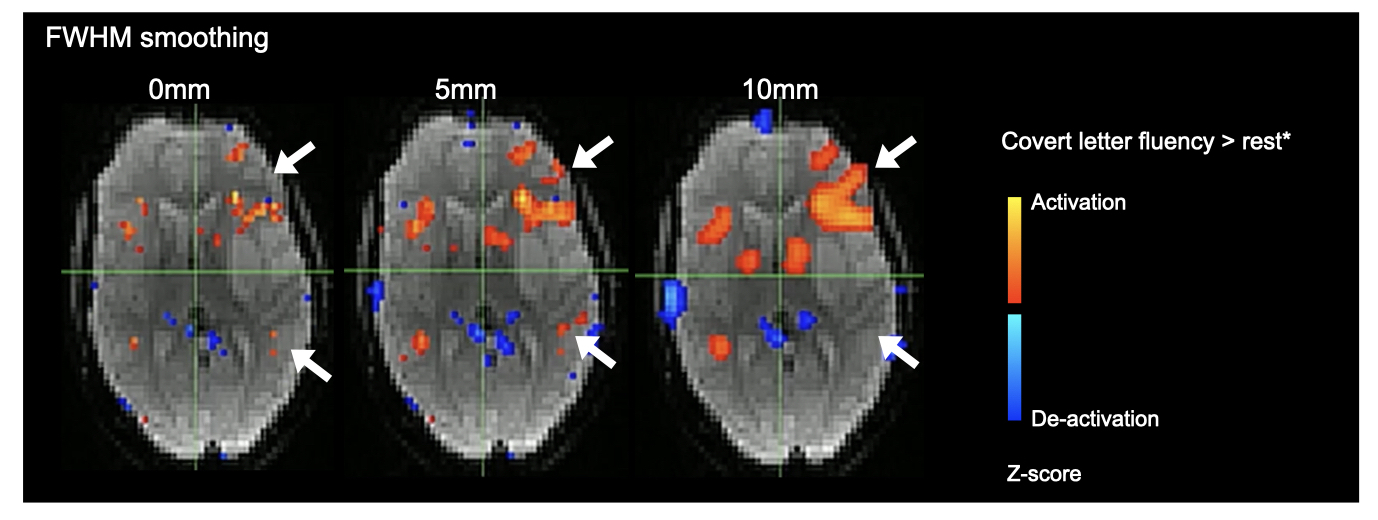
Spatial smoothing can improve SNR and statistical power in fMRI. However, this is only true if the extent of the smoothing is less than the size of the activations; large amounts of smoothing reduce the ability to detect smaller activations (Fig 8) and can spatially displace their focus.153 To retain spatial specificity in activation maps for presurgical clinical fMRI applications, the consensus of this Working Group is to avoid or minimize smoothing, using no more than 1 to 2 times the voxel dimensions,154 up to a maximum of 5mm isotropic FWHM (for a 2 to 3mm voxel dimension), but ideally 4mm. This recommendation minimizes the chances of blurring together noncontiguous cortical speech processing areas (e.g., for word production versus word hearing) identified 4mm apart using high density subdural electrode grids.155 This approach furthermore aims to balance smoothing as little as possible while retaining conspicuity of activations of interest (which can be more difficult to identify in unsmoothed data).

3.3.4. Registration of clinical FMRI and high-resolution structural images
Whenever fMRI results are overlaid onto an anatomical scan, it is important to identify and communicate any limitations in the underlying fMRI data, such as areas of susceptibility-related signal loss in fMRI (often affecting the inferolateral temporal lobe) which can lead to false-negative interpretations (e.g., in relation to a visual naming or reading task). Such misinterpretations can usually be avoided by first inspecting results in the original fMRI data space.
3.3.5. Data analysis and statistical inference
Meaningful clinical interpretation of fMRI data requires pragmatic knowledge of the advantages and pitfalls associated with the processing steps used for generating fMRI results.
Several commercial analysis packages exist for clinical fMRI analysis. These typically do not offer the user (m)any options to vary (or verify) parameters relating to statistical inference and thresholding. Therefore, in the wider community and among this Working Group, freely available research packages are commonly used, alongside clinically-licensed ones, for the added benefits the former provide.4,6 However, fMRI analysis packages developed for research use are typically not approved for clinical use and are optimized for a different use. An appreciation of the rationale behind analysis settings is important to understand why it is suboptimal to apply default recommended settings in some research fMRI analyses to clinical applications.
3.3.5.1. Hypothesis testing
The most common approach to analyze fMRI data - including clinical fMRI - is hypothesis-driven general linear model (GLM) fitting. A simple GLM implementation is available on many scanners and can be used to monitor fMRI scans in real-time. Real-time monitoring of activation maps while the patient is on the table can ensure that the collected data will be high yield and contain useful information for producing final fMRI activation maps (or allow the scan to be repeated with renewed instructions). Some members of this Working Group routinely supplement GLM-based analyses with data-driven spatial independent component analysis (ICA), which does not impose the same assumptions as the GLM (Appendix E).
3.3.5.2. Effect size maps, statistical thresholding and inference
Statistical testing and inference (including thresholding) constitute a major challenge for clinical fMRI. Thresholding turns fMRI results into maps of activation (or no activation), which guides the neurosurgical decision as to what tissue is potentially resectable (subject to intra-operative confirmation156) or should be avoided. However, currently, there is no standard or common approach that guides how to best threshold statistical fMRI maps for clinical purposes.
The first key step is to decide–among all the signals detected during the fMRI scan–which of the brain voxels or clusters of voxels show a signal that we are confident is related to the task (see Appendix E for elaboration on this critical topic). Selecting the appropriate statistical criteria to answer this question depends on assumptions about the (temporal onset, magnitude and extent of) fMRI signal measured, as well as choices about when we have statistical confidence in the detected activations. A false positive (FP) result – indicating more areas of activation than are truly there – could unnecessarily prevent surgery or maximal resection. Conversely, false negative (FN) results – where areas of language activity are erroneously ‘missed’ due to statistical choices – generally pose the highest concern in pre-surgical applications of fMRI. A false negative result in fMRI maps that is not interpreted with appropriate caution might result in surgical removal of an area of cortex that is crucial for language abilities. Consequently, choices in the statistical analysis of clinical fMRI data should be balanced towards avoiding FN (i.e., type II) errors. However, most widely used fMRI analysis packages are based on classical statistical inference that controls for FP rates, and are therefore not optimized (nor fully adequate) for clinical fMRI. Alternative statistical approaches are available that aim to control the balance between FNs and FPs (e.g.,157–161). However, these require broader validation. This working group particularly encourages the collection and pooling of such data / analyses across sites.
Once a task activation map has been generated, a second decision arises whether and how to threshold the resulting image. The magnitude of fMRI activation can vary substantially across individuals because of the effects of the lesion on the fMRI signal, different levels of performance/impairment,162 head motion and certain medications,163 among others. Appropriate thresholds differ for different individuals164 and choices need to be tailored to each patient. Our group recommends inspecting a range of statistical thresholds as well as the un-thresholded results both for every activation map, as well as task de-activations, in and around areas of interest for presurgical mapping. As a general principle, we recommend that established “institutional approaches” are reported clearly and evaluated rigorously against all available clinical data, most especially post-operative language outcomes.
3.3.6. Calculating laterality
Best practices in calculating laterality both in general and for clinical practice are still undefined.47 From a practical (analysis) perspective, the outcome of language laterality calculations with fMRI can change depending on the statistical threshold employed.165,166 Using a single fixed statistical threshold (i.e., not tailored to the individual) increases a risk of suboptimal or inaccurate assessment of fMRI language lateralization,167–169 especially when cognitive deficits or pathological features may reduce the overall magnitude (or height) of BOLD fMRI signals.165 Since language laterality is a continuum,170,171 the question of how to determine laterality based on fMRI is an important methodological challenge.
Many methodological variations to analyze fMRI language laterality have been proposed and evaluated against the Wada test (e.g.,21,44,168,172). However, the Wada test is itself not infallible (see41,173,174 and references therein). Consequently, the “ground truth” of language organization in the individual patient may not be absolutely known, with the result that the superiority of any one method of calculating a fMRI laterality index (LI) over the others remains undetermined. If LIs are generated, it is generally undisputed that LIs calculated at a single standard statistical threshold are not adequate,47 especially for clinical use. Additionally, a single ‘global’ LI is likely to be misleading in rare patients who have mixed dominance (e.g., anterior and posterior language areas in different hemispheres). In such cases, at any given threshold, laterality indices may be biased towards the non-affected hemisphere, limiting their utility. Consequently, when the clinical question is purely to establish relative lateralization to inform discussions around surgery, our recommendations are:
-
To include an appropriate range of tasks (and carefully consider task contrasts) to establish lateralization for the components of speech and language of greatest surgical relevance.
-
If LIs are calculated, visualize a range of LIs tailored to the patient’s levels (i.e., signal magnitude) of activation, or employ an LI calculation method that produces a weighted average across a range of thresholds (e.g.,175, see other approaches described in47).
-
Consider LIs from different language-related regions (not just the frontal lobe), but excluding regions involved in sensory (e.g., visual or auditory) or cognitive processes not specific to language (e.g., frontal eye fields, dorsolateral prefrontal cortex, anterior cingulate cortex).46
-
If the fMRI results are categorized (i.e., into ‘left-lateralized’, ‘right-lateralized’ or ‘mixed/bilateral’), indicate how these categories were defined (e.g., based on arbitrary LI cut-offs, or by comparison to specific population norms). Caution is advised in how atypical laterality is interpreted, noting high variations among experts in the meaning of ‘bilateral/mixed’ and ‘atypical’ dominance.47 Some clinicians might conclude from a non-nuanced fMRI report of a ‘mixed’ or ‘bilateral’ LI that surgery on the left hemisphere is without risk (e.g., interpreting this result as showing that both hemispheres are functionally equal), whereas such an interpretation is likely neither intended nor indicated, especially in patients with existing language impairments.
3.4. Reporting & interpreting fMRI results
Images are powerful. Great care should be taken to minimize misinterpretation, especially in terms of an apparent absence of activation near a susceptibility artifact, or when superimposing fMRI data onto structural images in which areas of artifact may be less prominent / invisible. Specific emphasis should be placed on limitations of a particular exam (e.g., regarding patient head motion, impairments, etc.). It is the opinion of this Working Group that if the person interpreting the data does not believe the report to be valid, no images should be generated at all.
fMRI reporting best practices have been proposed for the neuroscience community13 and complement guidelines for BOLD-fMRI dictation from the ASFNR (https://www.asfnr.org/wp-content/uploads/BOLD-fMRI-Dictation-Guidelines.pdf). Our Working Group recommends specific additions relating to the description of tasks and analysis methods used (Appendix G). Additional oral presentation of the fMRI findings, i.e., at surgical team meetings, offers valuable opportunities to highlight confidence and specific limitations of the results in an individual patient’s scan.
Importantly, while some surgical programs report using precise – but different – distance limits from fMRI activations to guide surgical margins,69 given skilled clinicians, extensive experience, and cautious interpretation, this approach is not likely to be accurate in most (if not all) cases, because distance calculations in fMRI are intrinsically related to preprocessing steps (especially smoothing) and statistical choices made by the user, rather than reflecting true functional boundaries.
4. Discussion
4.1. Summary
This document presents a summary of best practice recommendations from the OHBM Working Group on clinical language fMRI mapping. Our approach to generating these recommendations was based on the consensus and experience of this multidisciplinary committee, supplemented with the weight of available evidence behind clinical decision-making. Previous groups have reviewed a different range of clinical fMRI language applications and found different levels of validation for them. For example, the level of validation was higher for predicting language outcomes based on fMRI laterality assessments than for preventing deficits with MRI localization and tailored surgery, at least in epilepsy.5 Here, we further consider language tasks and task designs optimized according to specific clinical objectives. In doing so, we focus on specific patient populations (e.g., adult/pediatric) and possible modifications for their particular needs (for expanded considerations, please see https://doi.org/10.31219/osf.io/r7u8p). Putting forward recommendations based on the strongest available data remains challenging due to the absence of randomized controlled trials of language fMRI applied to most surgical populations. A second obstacle is the sparsity of studies conducting head-to-head comparisons of different tasks, and their performance when predicting post-operative language outcomes. There remains, therefore, a long way to go. Given these challenges, we place emphasis on language processes that should inform the selection of task fMRI, focusing on data that survive meta-analysis (predominantly for language lateralization) and converging lines of evidence from research neuroscience studies and surgical lesion outcome data (in the case of localization). We put forward practical guidance, based on state-of-the-art in neuroimaging science, for all aspects of clinical fMRI in relation to acquisition and analysis of individual patient data. Of course, our understanding of the basis of language in the brain, as well as technical implementations, continue to evolve. These recommendations do not aim to be final or prescriptive. Instead, our objective is to offer practical steps and guidelines for generating a shared knowledge base and collaborations which promote consistency in how fMRI language mapping is performed. In this way, this document aims to improve minimum standards and facilitate the objective assessment and quantification of the benefits, efficacy and limits of high-quality clinical fMRI. Achieving the latter requires thoughtful application to ensure that fMRI is:
- performed in a multidisciplinary manner, based on careful definition of individual patient characteristics and performance abilities
- backed by converging neuroscientific and clinical data
- follows best practices in data acquisition, processing and analysis
- is interpreted and used by the operating neurosurgeon based on interdisciplinary consultation
- systematically evaluated against clinical outcomes to determine added value for minimizing language-related risks
In this process, a clear need was identified for the wider reporting of individual groups’ experience in relation to fMRI, including relevant factors such as amount of ESM mapping required and duration of awake surgery based on fMRI predictions, and crucially, language outcomes. Some identified avenues for targeted developments and research, needed for language fMRI to substantiate and improve its clinical utility, propagation and availability, are detailed in Box 6.
4.2. Working Group’s position on the utility of clinical fMRI
An estimated 30-50% of European neurooncological centers49,176 and most (>90%) epilepsy surgical programs worldwide69 employ fMRI. A recent survey of US pediatric epilepsy surgery centers in the Pediatric Epilepsy Research Foundation Surgery workgroup found that 100% of surveyed sites were using fMRI for functional mapping, and more than 80 % also perform language mapping with implanted stereo-EEG-based ESM as an emerging approach to complement fMRI.177 Yet, justified uncertainty persists around fMRI’s ability to localize functions with the precision required for surgical planning. There are inherent constraints on the spatial precision that fMRI can achieve based on the limitations of the underlying BOLD contrast.178 Frequently cited confounds include the difficulty dissociating task-associated from language-essential neural activity with fMRI, and consequent variable sensitivity and specificity of fMRI relative to ‘virtual lesioning’ techniques.179
Evidence from epilepsy surgery candidates demonstrates the suitability of using fMRI as a surrogate for Wada testing to establish language dominance. As long as care was taken with task selection and design, fMRI has shown ability to predict postsurgical language outcomes to some degree. Measuring the effectiveness of language mapping in these scenarios remains difficult, perhaps impossible, in clinical studies in which the maps are used to adjust the surgical procedure, since there is no comparison showing what the outcome would have been without fMRI. As a result, the literature consists of mainly uncontrolled observations and the occasional comparison to historical control groups.
Cases of failure to prevent language declines likely exist, according to a recent clinical survey reporting the relatively common practice of resecting fMRI ‘activations’.69 Conversely, 17% of epilepsy surgical programs reported one or more cases where all language fMRI-positive activation was preserved, but a patient still suffered post-operative language decline (noting possible contributions of subcortical tract damage). None of these had been published. According to a recent survey on post-surgical care practices in Europe, not all neurosurgical centers refer each patient for neuropsychological assessments to evaluate language performance / outcomes. Some patient groups are particularly unlikely to undergo language evaluation; only 3% of patients with high-grade gliomas were offered language assessments after brain surgery, in comparison to 30% of individuals with low-grade gliomas.180 Practical challenges clearly arise in the neuropsychological scheduling and follow-up of patients who are on a rapid treatment pathway, or are due to undergo post-surgical adjuvant treatment. This appears to be less problematic in an epilepsy setting, where 70% of patients receive follow up.69 However, systematic, longitudinal outcome reporting is much needed to help inform what clinical questions fMRI is suited, or not suited to answer, and potential reasons for fMRI failures, if these are encountered.
In the opinion of this Working Group and with growing evidence of its predictive power, language fMRI mapping has the potential to add substantial value in the neurosurgical selection, consenting and planning of appropriately chosen patients. However, clinically meaningful fMRI mapping hinges on the precise identification of the surgical questions that fMRI is asked to inform, alongside careful characterization of patients to minimize fMRI studies in patients who are unlikely to benefit. It adds another layer of challenge for fMRI to provide ‘results’ when the question is poorly (or even not at all) defined beyond non-specific requests to “map ‘eloquent’ cortex”. Detailed knowledge and training are needed181 to evaluate fMRI results in the absence of “ground truth”, and meaningful clinical fMRI requires a highly interdisciplinary approach. When performed with due diligence and expertise, language fMRI mapping offers potential direct patient benefit. Examples of fMRI advantages include reducing the need for Wada testing,5 potentially enabling more aggressive or extensive surgical intervention when combined with tractography and ESM,182–184 and guiding optimal use of intraoperative stimulation182,185 and/or intracranial electrode placement,186,187 especially, but not exclusively, in pediatric patients.
4.3. Requirements for validation and standardization
Reservations surrounding the clinical use of fMRI language mapping are derived largely from comparisons with the Wada procedure (for language lateralization) and ESM (for localization). Previous reviews have summarized the highly variable rates of sensitivity and specificity reported when fMRI results are compared to these clinical standard techniques.21,42,188,189 There are reasons to be cautious about interpreting such direct evaluations, not only because of factors such as brain shift, but especially because of differences in what each technique reflects and how results from each tool are derived.
ESM is considered a clinical standard tool for the preservation of brain function during surgery but, like all techniques, has limitations (further considered in https://doi.org/10.31219/osf.io/r7u8p). Not all patients are able to tolerate190,191 or complete ESM.192 There remains little standardization in both how ESM is executed193 and how stimulation-induced language errors are interpreted.193,194 Importantly, preservation of all ESM-positive language cortex does not absolutely prevent enduring language deficits following epilepsy195 or tumor surgery, especially in high-risk locations such as the inferior parietal cortex (16.7% long-term deficits in one study96). Alternative methods, able to pre-operatively predict surgical risk and the likely safe(st) surgical approach, therefore retain an important role in neurosurgical planning. Among such methods, fMRI is most used, likely because it offers the greatest amount of spatial detail and does so non-invasively. However, fMRI specificity is per se limited compared to ESM. More areas are typically activated in fMRI than are associated with language errors during ESM, resulting in only modest overall specificity (approximately 55%-71%) when grouping across populations and approaches.189,196
It is important to contextualize these results: by temporarily evoking or inhibiting behavioral responses, Wada testing and ESM assess language function in fundamentally different ways from fMRI. Often, pre-operative fMRI paradigms do not probe the same components of language, or do so to different degrees than Wada and intra-operative ESM. For example, silent word generation tasks optimized to control for non-linguistic motoric aspects of word generation will by design not predict sites that cause speech arrest when stimulated intra-operatively.71 Instead, fMRI offers distinct advantages to evaluate crossed dominance for different aspects of language that are difficult to evaluate through Wada testing, and to explore language processing at the systems-level, including contributions of contralateral brain structures that are inaccessible to ESM. Neither Wada nor ESM preclude (long-term) postoperative deficits (e.g.,96,179,197,198). Still, the expectation – wrongly – prevails that correspondence between these techniques must achieve 100% for fMRI to be useful. Like others before us, we advocate that the clinical usefulness of fMRI should be evaluated in terms of its ability to anticipate and minimize (further) post-operative language decline, especially for patients unable to tolerate or complete awake surgery.190
In this regard, preoperative language fMRI mapping predicts postoperative performance on tests of naming5,199 and verbal memory5,199,200 in patients following dominant temporal lobe surgery for epilepsy. The predictive value for post-surgical outcomes appears superior for language laterality as determined by fMRI than by Wada,5,200,201 although these studies are hampered by varying approaches for interpreting the Wada, typically ignoring mixed dominance possibilities. In small case series, post-operative language deficits arose in patients whose resection area spatially overlapped with pre-operative fMRI activations202–204 even when no overlap occurred with positive ESM sites.198 Diverging results are also reported.205 A recent study reported better 3-year survival rates in high grade (but not low grade) glioma and metastasis patients operated with fMRI than without fMRI, irrespective of the use of ESM.206 This result was ascribed to greater surgeon confidence in undertaking extensive resections when guided by fMRI, as highlighted in previous reports.179 Thus, studies examining the predictive value of fMRI for avoiding postoperative language decline generally support fMRI’s complementary role in surgical planning. Still, no technique on its own is infallible and the best patient outcomes likely result from a combined approach.198 Reliability of speech and language fMRI mapping depends on the nature of the pathology and is likely to differ between epileptic lesions, brain tumors and vascular malformations. In high-grade brain tumors and high-flow AVMs, pathological vessels per se may only contribute within different limits to the oxygen supply of the parenchyma, somewhat restricting the use of fMRI (and Wada testing). Consequently, more comprehensive longitudinal evaluations of the applications that fMRI is particularly valuable for, and where its prediction failed, remain needed.
4.4. Vision(s) for improving clinical fMRI
International standardization of practice and reporting is needed to direct large-scale studies to objectively evaluate the long-term benefits of clinical language fMRI across neurosurgical indications. Emerging technological advances that offer higher resolution acquisitions, and the adoption of sophisticated preprocessing and analysis methods from the research realm, both hold promise for more precise localization of clinical fMRI results. Additional research is advocated to compare individual tasks head-to-head in terms of the strength and robustness of their associated activation patterns, and reliability in the context of patient performance difficulties. A particular limitation in validating language fMRI mapping is the sparsity of data in patients with atypical language organization. Due to the rarity of atypical language dominance, reports to date have largely consisted of case studies or very small case-series from which it is difficult to draw firm conclusions as to the accuracy and limitations of fMRI. Additionally, few studies have investigated how common medications, such as antiepileptic and antiedematous drugs (e.g.,207–209), may adversely affect BOLD fMRI. Finally, since all clinical tests carry some level of error, further consideration should be given to the level of evidence required to evaluate fMRI as a clinical standard for select indications. We propose this discussion should move towards detailed evaluation of pre- vs post-operative speech and language deficits, as determined through patient-reported and validated, standardized neuropsychological outcome measures across the wide range of patient populations routinely undergoing clinical fMRI.
Data and Code Availability Statement
Not applicable.
Funding Sources
No specific funding was available for this consensus work.
Conflicts of Interest
The authors have no conflicting interests to declare
a Critical, often called “eloquent”, which is, strictly speaking a mereological fallacy according to Bennet & Hacker,210 and also used in a much broader sense in the neurosurgical community.211
While it is generally interhemispheric dominance for language (and verbal memory) that is sought to be established prior to esp. epilepsy surgery, traditionally by (super-)selective Wada testing, it is the asymmetrical lateralization of activations that can be established by fMRI. Although fMRI cannot discriminate indispensable from expendable activations per se (and at the individual patient level), lateralization has been shown to be a useful surrogate to predict postsurgical outcome in sufficiently large patient samples.