Simultaneous multi-slice (SMS) or “multiband” (MB) acquisitions1 for EPI data have become popular and wide-spread methods over the last decade. This technique uses a multiband radiofrequency excitation pulse to resonate multiple slices simultaneously, and the reconstruction algorithm exploits the known features of array-receiver coil geometry to separate the signals from each slice location.2,3 The effect is to accelerate the acquisition of a volume by a factor equivalent to the number of slices acquired simultaneously i.e. a MB factor of two halves the acquisition time, and a MB factor of four acquires a volume in a quarter of the time.1 Extremely high acceleration levels of up to 16 times have been demonstrated with 7 Tesla MRI scanners.4 Multiband methods are independent from older parallel imaging acceleration methods such as GRAPPA and SENSE,5 and can be used in combination with them for an additional boost in speed.6
This acceleration enables a number of possibilities for design of fMRI acquisition sequences. Most obviously the TR (repetition time, or time to acquire a single volume) can be strikingly reduced from a more standard range of 2-4 seconds on modern scanners, to just a few hundred milliseconds. Alternatively, the number of slices and/or the spatial resolution can be increased in order to achieve a larger field of view or smaller voxel sizes, while still maintaining a reasonably short TR. With high levels of MB acceleration essentially both can be achieved; a large number of relatively high resolution (e.g. 2x2x2 mm, or even smaller voxels) slices can be acquired for full-brain coverage, while still achieving a much shorter TR (i.e. < 1 second) than typical with standard single-band sequences.
This was the approach taken by the Human Connectome Project (HCP) for their resting-state scans.7 The HCP sequence used a multiband acceleration factor of 8, with 2x2x2 mm voxels in a 104x90 matrix and 72 slices. With this high level of acceleration they were able to achieve a TR of just 0.72 seconds. This general approach to sequence design has been highly influential and other large-scale imaging projects have adopted similar approaches for their functional imaging. These include the Adolescent Brain Cognitive Development study,8 the Baby Connectome Project,9 the third phase of the Alzheimer’s Disease Neuroimaging Initiative,10 the Chinese Human Connectome Project,11 the Japan-based “Brain/MINDS beyond” project,12 and the UK Biobank13 among others. To facilitate wider adoption, the HCP has even published a primer on the “HCP-style paradigm” for human neuroimaging.14
There is no question that these large-scale projects, which scan many hundreds or thousands of subjects, have been hugely significant in progressing the entire research field, and novel insights and results are being derived and presented from these vastly rich, openly-available datasets almost on a daily basis. However, the majority of fMRI researchers are not working within this kind of paradigm and are performing more ‘everyday’ imaging work in relatively small-scale studies. A survey of the literature for 2017 and 2018 found that the median sample size in fMRI research was 23-24, and median sample size increases by roughly 0.74 per year.15 Assuming that rate of increase has still held since 2018, the median sample size at the time of writing should now be around 27-28. In my own research area (pharmacological fMRI), the difficulty, complexity, and cost of the studies often means that sample sizes are well below this.
It is difficult to estimate the influence of the HCP approach to fMRI sequence design on these smaller-scale ‘everyday’ projects that form the majority of fMRI research, however anecdotally, there is a strong awareness of the HCP protocols within the fMRI community. The wider availability of modern scanners with high-power gradient systems (e.g. Siemens Prisma or Skyra, GE Signa, and similar systems) and equipped with 32 or 64-channel head coils has enabled many labs to implement HCP-like multiband sequences, and the growth in papers which contain the terms “multiband” and “fMRI” (from 37 entries in 2010, to 1,540 in 2022[1]) suggest multiband sequences are currently popular. My purpose in this editorial is to sound a note of caution about the widespread adoption of HCP-like multiband sequences and argue that (while they are certainly ‘good’ sequences in many ways) they may be far from optimal for typical smaller-scale experimental studies. Experimental power, reliability, and replicability are crucial issues in fMRI research16 and are dependent on a number of factors including the underlying reliability of the tasks/measures,17,18 the balance between the number of subjects and the number of trials/length of scans acquired per subject,19,20 magnetic field strength,21 and the features of the acquisition sequence. Since many of these factors (e.g. subject numbers) may be sharply constrained by the resources available for any given project, or in the local area (e.g. availability of high field-strength scanners), it is therefore vital to optimize the factors which are relatively easily controllable, such as the acquisition sequence.
The first feature to consider for multiband HCP-like sequences is the voxel size. Triantafyllou et al. (2005) demonstrates that BOLD signal-to-noise ratio (SNR) scales linearly with voxel volume at all three commonly-used field strengths (1.5T, 3T, and 7T).22 What this means is that a relatively small change in voxel dimensions (i.e. from 3 mm isotropic to 2 mm) represents a more than three-fold drop in volume (27 mm3 to 8 mm3), with a concomitantly large drop in SNR. The main reason for using high-resolution (2x2x2 mm) acquisitions in the HCP is stated clearly in Smith et al. (2013), namely that they wished to optimize the acquisition for cortical surface-based analyses, where smaller voxels have a number of benefits. The authors acknowledge that small voxels have poor SNR, but that this is ameliorated by the decision to acquire a solid hour of resting fMRI data from each subject. Small voxels therefore made eminent sense in the HCP (and similar projects) where a large amount of data was collected from many hundreds of subjects and experimental power was therefore very high. Most smaller-scale studies collect perhaps less than 10 minutes of resting data from each subject, where in fact a somewhat longer acquisition (up to 15 minutes, or even longer) is likely more optimal.20,23 For such studies, that also intend to use standard volumetric analyses, voxel size is a critical determinant of SNR and therefore experimental power, with small voxels likely to have markedly deleterious effects. Pre-processing pipelines for volumetric analyses typically include a spatial smoothing step, where a Gaussian filter of up to 10 or 12 mm (FWHM; Full Width at Half Maximum) is applied, with an optimal value for group-level inference perhaps around 8 mm FWHM.24 Clearly, acquiring high-resolution data with low SNR makes little sense if the resolution is subsequently severely degraded with a large smoothing kernel in the pre-processing pipeline.
The second major issue is the temporal resolution. At shorter TRs, SNR is exponentially lower due to the reduced T1 recovery which can occur within the TR.25 At TRs below 1 second, T1 effects are clearly more evident, with reduced contrast between the white and grey matter. This may also mean that registration algorithms intended to correct head-motion or to register functional data with anatomical images are compromised and less accurate.7 While TRs of around 1 second may be beneficial for statistical detection of effects compared to longer TRs of 3-4 seconds,26 the drop in SNR with very short TRs (<1 second) will likely nullify this benefit. A TR of ~1000±200 ms is likely to be the optimal range for many studies.27,28 The signal conventionally being measured (the Haemodynamic Response Function; HRF) is a slow signal that evolves over a period of ~10-15s (though recent work has highlighted somewhat faster processes, particularly in response to brief stimuli; for a review see29). Extremely fast sampling therefore provides little intrinsic benefit for conventional analyses using a canonical model of the HRF, especially with the concomitant drop in SNR. As noted above, the HCP protocol used a TR of 0.72 seconds, but the effects of this decision on SNR and experimental power are also compensated for by the large amount of data collected per subject, and the large number of subjects. As for spatial resolution, smaller-scale studies should seek to optimize temporal resolution with an emphasis on SNR, experimental power, and reliability.
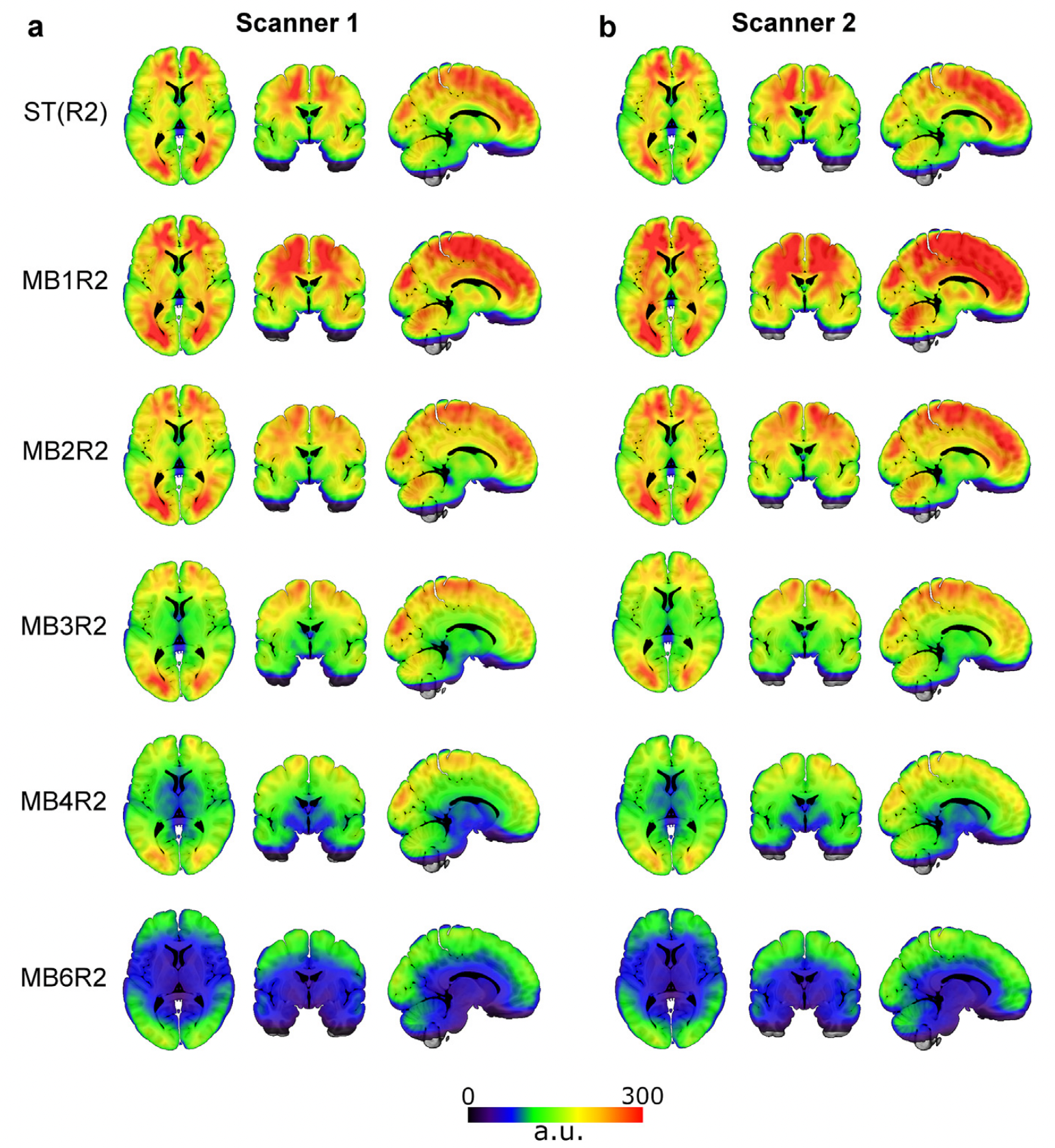
The third major issue with these sequences is what enables the first two; the high level of multiband acceleration. Multiband sequences introduce additional noise signals into EPI images which have a characteristic striped or checkerboard pattern.30 There are also ‘slice-leakage’ effects6 where signal from one slice is artefactually manifested in another simultaneously excited slice. Replicable intra-slice artefacts have also been demonstrated where movement of the eyes or blinks manifest as signal distortions at predictable locations in the brain.31 A further undesirable effect is general signal dropout in medial/ventral regions of the brain,27 meaning that sub-cortical (thalamus, striatum) and medial-temporal (amygdala, hippocampus) structures are poorly imaged (see figure 1). This effect has been most clearly documented by Srirangarajan et al. (2021) who demonstrate that multiband sequences are generally worse than single-band sequences at detecting task-related activity in the ventral striatum. Multiband artefacts may also interact with head-motion to produce additional artefacts in a potentially non-linear manner.7,32 All these factors are likely more problematic at higher acceleration levels.

To summarize, the HCP acquisition sequence is a relatively high-resolution, but low-SNR, sequence because of its use of small voxels, a short TR, and high levels of multiband acceleration. This was compensated for by acquiring an hour of resting fMRI data for each subject and scanning a very large number of subjects (more than 1000). The decision to use small voxels in the HCP is justified by the intention to use cortical surface-based analysis methods,7 though the justification for such a short TR and MB=8 acceleration is perhaps less clear. This was a sequence that was designed to provide optimal performance for a particular use-case. Its adoption by other large-scale imaging efforts with hundreds of subjects (and similar aims) is also entirely reasonable. However, it is very unlikely to be optimal for the majority of fMRI research where shorter scans are acquired, with ‘typical’ (N=20-30) subject numbers, and with ‘standard’ (volumetric) analysis methods. For such studies considerations around signal stability, SNR, and experimental power should be absolutely paramount when designing the acquisition sequence. It should be noted at this point that the use of multiband acceleration per se is not the issue; the real problem is pushing acceleration and resolution to levels where artefacts and/or noise signals dominate the variance in the time-series. There are also, of course, many ways to design a ‘bad’ fMRI sequence that will yield poor BOLD contrast (e.g. high levels of slice-based acceleration, very short echo times) that do not involve use of multiband.
When my local MRI facility first implemented multiband sequences for fMRI we undertook fairly extensive testing on both our 3T scanners, documented in.27 We found definite benefits of multiband acceleration on statistical outcomes, particularly for resting-state data, but higher levels of acceleration had significant negative effects on tSNR. Based on this testing, we decided that a much more conservative use of multiband was most appropriate for our particular ‘typical’ study (pharmacological studies, often with relatively small subject numbers). We settled on a functional sequence using 2x multiband acceleration (combined with GRAPPA=2) with 3 mm isotropic voxels, and a 1.25 second TR. We felt at the time that this provided a modest, but still useful, level of acceleration, while minimizing other undesirable effects (T1 saturation, image artefacts, signal dropout, etc.). Our results and the sequence we implemented were broadly in accordance with others who have documented similar testing data.6,28,33 This sequence has been successfully deployed in a number of projects34–41 but we have also modified it on occasion to suit particular studies, for example using thinner 2 mm slices to reduce susceptibility artefacts in ventral brain regions.42,43 My intention here is not to advocate for the use of this particular set of sequence parameters, or any other set, but to recommend that individual researchers think carefully about their use of multiband and do appropriate testing and development work. The optimal sequence for a particular project depends on a great number of factors, including the study endpoints, brain regions of interest, analysis approaches, the number of subjects, and the tasks or paradigms involved. An additional crucial consideration is the hardware available, with some array receiver coil configurations putting crucial limits on the acceleration level,44 and field strength (3T vs. 7T) also likely shifting the optimal trade-off point between resolution and experimental power.45 Researchers need to think carefully about all these factors, collect pilot data, examine it carefully, and design acquisition sequences accordingly. Temporal SNR measures are simple to calculate for pilot data, and provide crucial information when comparing different sequences, either on MRI phantoms, or live-subject pilot data. A number of software packages are also available which can calculate tSNR and provide a range of other useful quality-control checks.46–48 In some cases this process may mean abandoning use of multiband sequences altogether49,50 and perhaps considering alternative means of increasing SNR such as multi-echo sequences.20 Multi-echo sequences which incorporate a range of TE data may be particularly useful for iron-rich sub-cortical regions51 where susceptibility effects mean that signal may be poor with typical TEs of 30-35 ms, particularly in older subjects.52
Conversely, higher (spatial) resolution and short TR values achieved with relatively high multiband acceleration levels may be a good choice for particular projects. In such cases the cost/benefit analysis shifts in favor of higher resolutions instead of SNR. For example, smaller voxels (with minimal or no smoothing applied) are likely optimal for visualizing the response patterns of cortical columns,53 or when imaging subcortical structures such as the basal ganglia.54,55 Even for cortical regions, applying advanced processing techniques such as cortical surface-based smoothing may also mean that voxel size can be reduced while maintaining high levels of signal detection ability.56 Regarding temporal effects, there is a growing body of work which suggests that BOLD responses may happen much faster than the standard model of the HRF. Responses to stimuli as short as 5 ms have been demonstrated,57 as well as dynamic prediction-related activity in the visual cortex which evolves over time-scales of less than a second.58 Coherent BOLD activity has also been demonstrated to stimuli that oscillate at up to 0.75 Hz, strongly suggesting that BOLD activity can (at least under certain conditions) modulate significantly faster than the standard HRF model would predict.29,59 Some work has even suggested that there may be information content related to resting-state network dynamics at higher frequencies of up to 1.4Hz.60 Higher resolution sampling with short TRs has been a crucial method in documenting all these novel effects. Another important application of faster sampling is in characterizing physiological signals such as cardiac and respiratory effects, or high-speed vascular dynamics.61 Both high spatial and temporal resolutions might therefore be a reasonable choice in small regions where physiological noise is a particular issue (for example, brainstem nuclei62). For all these applications, multiband acceleration may be extremely useful in achieving the desired spatial and/or temporal resolution, and the trade-off considerations with SNR in these specialist applications are likely to be somewhat different than in more ‘standard’ experimental approaches.
Multiband sequences have been a hugely significant step in the ongoing development of modern acquisition sequences for fMRI, but they are not a panacea, and (as with any aspect of MRI sequence design) they involve trade-offs and compromises. The paradigm used for functional imaging in the HCP has been highly influential, but is unlikely to be optimal for researchers working on smaller-scale studies and/or with different subject groups (e.g. clinical patients, children), as the high-resolution approach can badly compromise SNR. High spatial resolutions are redundant for standard volumetric group-averaging analyses as the data is effectively down-sampled by spatial smoothing, and high temporal resolutions are also generally not required (outside of specialist applications) because of the relatively slow signal (the HRF) being sampled. Injudicious use of highly-accelerated, relatively low-signal sequences can have a potentially disastrous effect on data quality, and lead to much wasted time, effort, and resources. Multiband sequences can be extremely useful tools and have enabled important developments in high-resolution imaging, but they need to be used prudently, and with a keen eye on optimizing acquisition parameters for a project’s specific goals.
Source: Google Scholar, search term of “multiband fMRI” conducted on the 1st of October, 2023.